Clinical Case Presentation January 2024
- Malaysian Society of Geriatric Medicine
- Dec 28, 2023
- 3 min read
Chee Sing Hui
Supervisor: Dr Alan Ch’ng Swee Hock
Current Posting: Hospital Seberang Jaya
Case Scenario
Mr T 78 years old gentleman
Underlying
1. Diabetes Mellitus
2.Hypertension
3. Dyslipidemia
4. History of right neck of femur frature, post right short PFN in 2018
Under KK Butterworth follow up
Previous medications
T. Atenolol 50mg OD
T. Gliclazide MR 60mg OD
T. Mecobalamin 500mcg OD
T. Perindopril 2mg OD
T. Metformin 1g BD
T. Simvastatin 40mg ON
Premorbid
Well, ambulating without aid, no history of fall after 2018
bADLand iADLindependent. Able to drive car around, able to watch TV
No cognitive issue, no depressed mood, no incontinence.
Has hearing impairment
Bilateral knee OA
Past admission
Admitted to Private hospital for 3 weeks before admitted here in Hospital Seberang Jaya
Treated there for Klebsiella pneumonia bacteremia
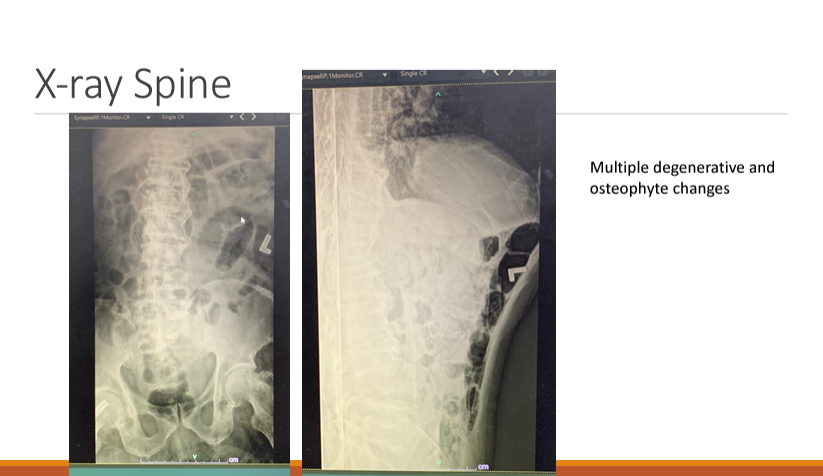
Done USG abdomen, Chest and spine x-ray, which showed multiple osteophyte over spines
Was discharged with
Upon discharge he lost his ability to walk, appetite was poor, back pain, enervated and debilitated requiring full support from his wife
Presenting illness
After 2 weeks at home, he started to have
Shortness of breath
Productive cough
Altered
Presented to ED HSJ on 25/10/23
BP 101/54, PR 84, Spo2 93% under room air, Temp 36.9c, Reflo(DXT) 5.1
Alert, responsive, but appeared lethargic, delirious
Lungs bilateral lower zones crepitation
CVS no murmur
Per abdomen soft, non tender no mass felt
Power Upper limbs: 4/5, lower limbs 3/5
Chest x-ray

Blood ix
TWC 78
Hb 10.4
Plt189
ABG under room air: pH , pO2 64.6, Lac 2.5, HCO3 25.9
CRP 196
Urea 8.6, Na 122, K 4.5, Create 123
Blood ix
Blood C&S on 26/10:
Klebsiella pneumonia
Sensitive: Amikacin, Augmentin, Unasyn, Ceftriaxone, Cefuroxime, Gentamicin
Resistance: Ampicillin
Diagnosis
HAP with Klebsiella pneumonia bacteremia-Partially treated
AKI and transaminitis(resolving)
Hypoactive delirium
NCNC anemia
Treatment
Patient was given IV Unasyn 3g TDS
Npo2 3L/min
For USG abdto look for collection
ECHO to look for vegetation
R9J8MH6t3BYCPXMFLa35R7aUJV9i4siPhX
Blood ix

Blood culture
Ultrasound was quickly done on 26/10/23 which showed no collection,
Seen by ophthalmology team on 30/10: No evidence of endophthalmitis,
ECHO was done on 1/11/23 which showed no vegetation.
So...
After 1 week of IV Unasyn
Patient still lethargic, not orientated to place. 4AT score 7. Body generalised swelling.
Patient remained afebrile
He managed to wean off oxygen
Inflammatory markers decreasing
Are you happy with the current treatment?
Most of the non-ESBL Klebsiella Pneumonia bacteremia would’ve been discharged after completed 1 week of antibiotics

Blood culture
Repeated blood culture on 4/11/2023:
Klebsiella pneumonia
Sensitive: Augmentin, Unasyn, Ceftriaxone, Tazocin, Cefoperazone, Cefepime, Gentamicin
Intermediate: Unasyn
Resistance: Ampicillin, cefuroxime, Co-trimoxazole
IDR on 1/11/2023
Input from physiotherapist: Patient showing bilateral hamstring tightness, more stiff over left lower limb, can sit but lower back pain limiting his posture, can sustain less than 5 mins only. The pain was radiating from back to leg
X-ray spine showed multiple osteophytes from L1-5
Modified Barthel Index: 54
Plan
Restart T.Pregabalin75mg BD
Add Ketoprofen patch 1/1 OD over lower back
Encourage bed mobility, sitting up and prop up patient
IDR on 1/11/2023
During the IDR, we suspected spinal pathology
CT Abdomen Pelvis was done on 9/11/2023
L3/L4 infective spondylodiscitis associated with anterior paraverterbral collection, multiple multioloculated, multiseptated intramuscular collections are seen involving left psoas (5.2x3.2x13.3) and right psoas (5.2x2.6x13.6), right iliacus (4.6x5.2cm) muscles extending to right iliopsoas muscle at the upper thigh and right pectineus muscle (1.8x4.4cm) and right posterior subphrenic loculated collections (2.9x4x4.3cm)
Cholelithiasis
Bilateral pleural effusion
MRI lumbosacral spine (11/11/23)
Spondylodiscitis involving L3/L4 and L4/L5 levels with evidence of extension to epidural region, extensive multiloculated abscessessinvolving pre-and paravertebral muscles, as well as bilateral psoas, iliopsoas and illacus muscles.
L5/S1 disc bulge causes moderate bilateral subarticular recess narrowing, mild bilateral neuroforaminal narrowing and spinal canal stenosis
MRI Lumbosacral spine

Diagnosis
Invasive klebsiella pneumonia
Hypoactive delirium, deconditioning
NCNC anemia
Treatment
Drainages were inserted bilaterally into the psoas muscles
IV Unasyn for 4-6 weeks
Repeat CT TAP later to look for resolution of abscesses
Spine –Conservative treatment
Rehabilitation
Nutrition
Bedsore prevention
Discussion
How is this Klebsiella Pneumonia different from typical Klebsiella pneumonia infection.
Is delirium expected in this patient?
This case is typically an atypical presentation of illness in Geriatric patients we see everyday. What are the risk factors of atypical presentation in this case?
Warning signs
- High TWC and CRP despite 1 week of treatment
- Persistent radiating pain from the back to the leg
- Persistent klebsiella pneumonia from blood cultures
Red herring
- Rather "clear" ultrasound abdomen - Which could be operator dependent
- A partially treated klebsiella pneumonia from Private Hospital - one would always falsely presume that private hospital would have thoroughly carried out a batteries of investigations and imagings, providing hi-fi treatments
- A false presumption of hypoactive delirium can be dangerous at times, be sure to thoroughly investigate if patient still appear ill despite adequate treatment
- Multiple osteophytes from L1-L5 giving false presumption of the cause of his sciatic pain
Klebsiella Pneumonia
The klebsiella organisms have…
Presumably spinal pathology was suspected from the beginning, but reluctance to conduct MRI had occurred due to resource limitations or ageism. I guess one would argue for low threshold for MRI scans in such situations in the future.